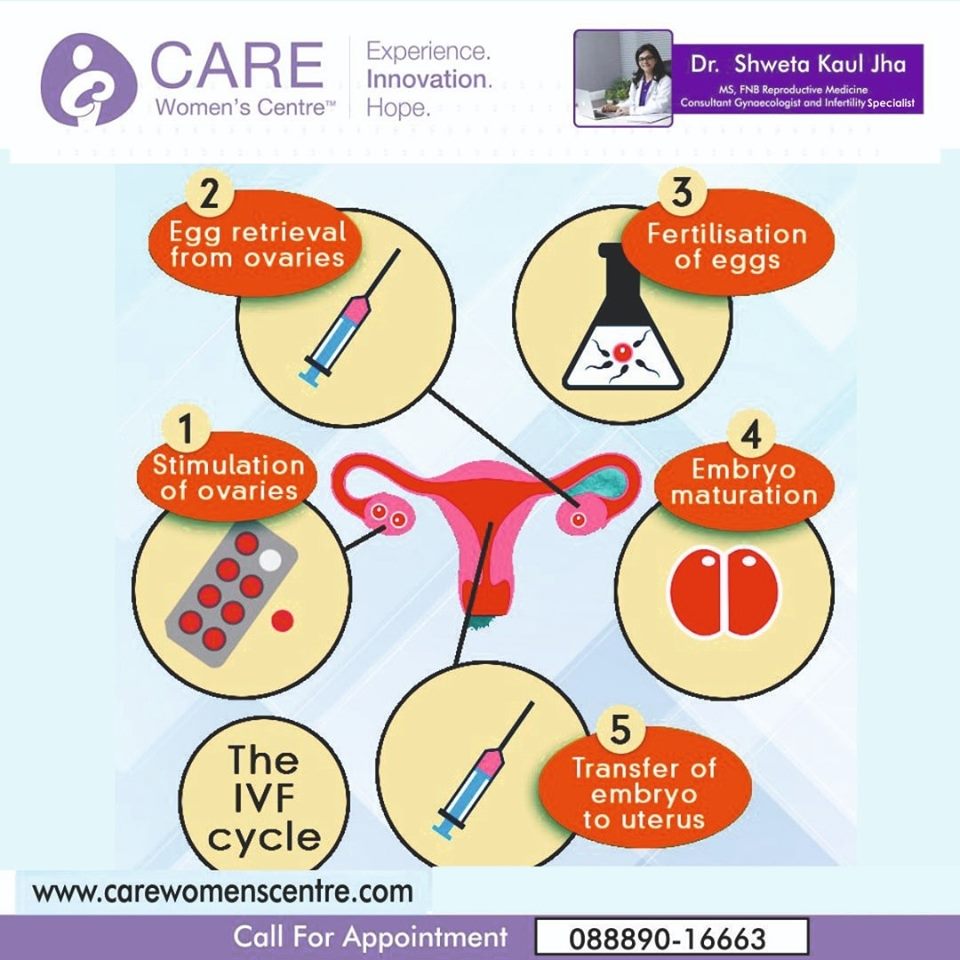
New hope for childless couples, now IVF treatment available at affordable cost. Having a child post marriage is a very important part of life. The pain of not having a child is only felt by parents who cannot conceive. Infertility is a global problem affecting millions of people. Making babies is now possible for more childless couples at Care Women Centre Indore. With the treatment available now, more such couples will be able to welcome their babies home For more information, kindly call: 88890–16663 or visit www.carewomenscentre.com for more details.
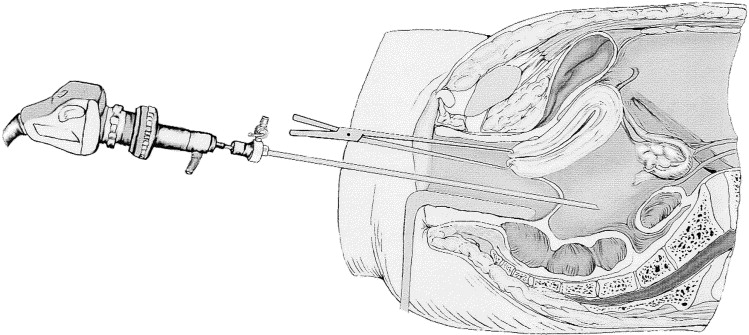
Transvaginal hydrolaparoscopy is a culdoscopic approach for the inspection of the posterior pelvis, but, in contrast to culdoscopy, uses an aqueous solution for the distension of the pelvic cavity and small diameter optics. The technique is used for diagnostic purposes in patients with infertility and is performed under local anesthesia or conscious sedation in an ambulatory surgical center. We report on a continuous series of 1,000 patients with infertility and without obvious pelvic pathology. Access and good visualization was obtained in 96.8% of the patients. The main complications were intraperitoneal bleeding and bowel perforation, which after the initial period occurred respectively in 1.9 and 0.1%. All complications were managed conservatively, and no major complication occurred. Clinically significant pathology was diagnosed in 25% of the patients, which allowed immediate triage of the patients for further management. Transvaginal hydrolaparoscopy can be proposed as a first line technique to replace hysterosalpingography and diagnostic laparoscopy in the exploration of patients with unexplained infertility.
Introduction
In Europe over the past 40 years, endoscopic evaluation of the pelvis has become an integral part of the infertility work-up. In routine practice, hysterosalpingography (HSG) is the first-line investigation and, if normal, laparoscopy is frequently delayed for 6 months or more. Laparoscopy is indeed an invasive procedure, associated with potentially serious complications, and together with hospitalization it can also be an expensive procedure. On the other hand, HSG is inferior to the chromopertubation test for the diagnosis of tubal patency [1] and also has a low sensitivity for the diagnosis of pelvic endometriosis and adhesions. If laparoscopy is performed as a first-line investigation on all infertile patients, there will be a large number of patients with normal findings or with minor pathology that has no or doubtful impact on the management of infertility.
It has been argued that with the advent of ART, laparoscopy can be omitted from the infertility work-up when there is no abnormal contributing history and the HSG is normal and, as a consequence, the cost of fertility treatment is reduced without compromising success rates [2]. Karande et al. [3], however, found in a prospective randomized trial that a higher pregnancy rate with lower costs is achieved with a traditional treatment algorithm than with IVF-embryo transfer as a first line-therapy.
We therefore wish to report on a continuous personal (H.V.) series of 1,000 procedures of transvaginal laparoscopy (THL), which were performed in combination with the mini-hysteroscopy and chromopertubation test as a first-line investigation of female infertility [4]. The combination of the three procedures has been coined transvaginal endoscopy (TVE).
Materials and methods
THL was discussed with all women who met prospectively established exclusion and inclusion criteria. In all patients, the indication was primary or secondary infertility. The patients had a complete history, physical examination and transvaginal sonography. Patients were excluded if they had an indication for operative laparoscopy, abnormal pelvic findings such as fixed retroverted uterus, rectovaginal endometriosis, large ovarian cyst or obliterated cul-de-sac, or an upper vaginal stenosis. Patients with vaginal or pelvic infection were first treated before THL was performed.
THL was used as described by Gordts et al. [5]. With the patient in the dorsal decubitus position, only a limited amount of fluid is required to have the tubo-ovarian structures floating in the excavation of the posterior pelvis. We used a narrow-diameter (<3.5 mm), foroblique 30°, wide-angled and rigid optic, a high intensity light source and a digital camera. Inspection of the pelvic structures was achieved without grasping or manipulation. At the end of the procedure a chromopertubation test was performed and, when indicated, salpingoscopy was added. All interventions were performed under conscious sedation as an office procedure in an outpatient surgical suite.
Transvaginal laparoscopy was considered complete if the tubo-ovarian structures, pelvic sidewalls and cul-de-sac could be seen, or if pathology was diagnosed that indicated the need for operative intervention or ART.
Results A total of 1,000 THLs were performed during the period starting from 1998 until 2003. Thirty-two (3.2%) failures occurred with failed access in 11 (1.1%) and absent or poor visualization in 21 (2.1%). In total, 968 (96.8%) of the procedures were completed. No pathology or pathology of minor clinical significance was found in 736 (76%). In the group with completed procedures, unexpected clinically significant pathology was diagnosed in 240 (25%) and included mainly ovarian endometriosis, tubo-ovarian adhesions, isthmic block and hydrosalpinges. The diagnostic findings resulted in 36 (3.7%) operative laparoscopies and 204 (21.1%) medical therapies and ARTs.
No major complication occurred in this series. Intraperitoneal bleeding was seen in 23 (2.3%) of the patients and occurred on the posterior wall of the uterus (n=13), parametrium (n=2), ovary (n=2), omentum (n=1) and adhesions (n=5). Bowel perforation occurred in 5 (0.5%) and was managed conservatively with antibiotics. Infection occurred in two (0.2%).
The correlation of the failures (no access or no visualization) with the experience showed that 5 (10%) failures occurred in the first 50 procedures and 26 (2.8%) in the subsequent 950 procedures (P=0.018). Bleeding occurred in 5 (10%) of the first 50 cases and 18 (1.9%) of the following 950 cases (P=0.004). Bowel perforation occurred in 4 (8%) of the first 50 cases and in 1 (0.1%) of the following 950 cases (P<0.0001).
Discussion
By using TVE as a first-line investigation of female infertility, we avoided HSG in 96.8% and laparoscopy in 93.2% of the patients. In 24% of the patients, unexpected major pathology was diagnosed and recommendations for operative laparoscopy, medical therapy or ART could be made.
Several studies have validated the feasibility, reproducibility, diagnostic accuracy, acceptability and safety of the procedure [6]. Different centres have reported access in over 95% and normal findings in 41 to 59% of the cases. In this series of 1,000 consecutive cases, access and visualization of the pelvic structures were achieved in 96.8% of the patients. The performance of THL is defined by visualization of the ovaries, fallopian tubes, posterior wall of the uterus, ovarian and uterosacral ligaments, sidewall of the posterior pelvis and cul-de-sac. In this series, these structures were normal or showed pathology of minor significance in 76% of the patients.
The potentially serious complication of transvaginal access is rectal perforation and sepsis. In a survey of 3,667 procedures the incidence of bowel perforation was 0.65%, which decreased after the initial experience to 0.25%. No delayed diagnosis and sepsis occurred, and 92% of the cases were managed with outpatient antibiotics [7]. In the present series minor bleeding occurred in 2.5% and bowel perforation in 0.5% of the patients. Analysis of the occurrence of complications in function of experience confirmed the importance of the learning curve. After the initial 50 cases, the complication rate of intraperitoneal bleeding and bowel perforation decreased significantly to 1.9 and 0.1%, respectively. It should, however, be noted that even in experienced hands these complications can occur and, therefore, the patients need to be informed. However, in this series no major complication such as sepsis occurred and, similar to previous series, most bowel perforations were managed conservatively with antibiotics without consequences.
As a first-line procedure for the investigation of female infertility, TVE is in direct competition with HSG. The prognostic value of the chromopertubation test has been shown to be better than that of HSG [1]. Four authors reported abnormal findings at THL in 44% of 241 patients with normal or suspected hysterosalpingography [6]. Shibahara et al. [8] compared HSG versus THL in a series of patients with and without a history of Chlamydia infection and found that THL was superior for the diagnosis of peritubal adhesions. The additional advantage of THL for tubal exploration is the ability to examine directly the tubal mucosa by salpingoscopy. Salpingoscopy is a better predictor for pregnancy outcome after tubal reconstructive surgery than routine investigation by HSG and standard laparoscopy [9, 10].
Fatum et al. [2] suggested that in patients with a normal HSG, laparoscopy would be superfluous and patients should undergo up to six cycles of gonadotropins and IUI and then undergo IVF if they continue to be infertile. However, in a recent study Capelo et al. [11] found significant pelvic pathology in one third of the patients failing to conceive after four ovulatory cycles of clomiphene citrate and concluded that early endoscopic diagnosis of such pathology would have allowed the couple to proceed directly to IVF.
Cicinelli et al. [12] found in a randomized controlled trial that THL in combination with mini-hysteroscopy in an outpatient setting was better tolerated by the patients than HSG. Finally, HSG is a diagnostic X-ray procedure that exposes the bladder, ovary and colon to radiation. The organ-specific radiation doses of HSG for the bladder and colon are estimated at 4.67 and 2.82 mGy, respectively. It is now generally accepted that there is no threshold dose below which radiation exposure does not cause cancer, and the attributable risk of diagnostic X-rays is estimated to range from 0.6 to 1.8 of cases of cancers per year [13].
When an accurate infertility exploration can be performed with a minimally invasive procedure and a reliable treatment exists, an early diagnosis followed by the most appropriate, effective treatment can greatly reduce the monthly failures and the sense of frustration for the couple, particularly when age and time are additional unfavorable factors.
Our current approach of exploring female fertility after 1 year or more of infertility may paradoxically lead to undertreatment as well as overtreatment.
Recent prospective population-based studies have demonstrated that the time to clinical pregnancy in most women with normal fertility is not more than 6 months [14, 15]. It can therefore be assumed that already after six cycles with fertility-focused intercourse, irrespective of their age, most women with normal fertility have conceived and that the remaining group is largely composed of couples faced with subfertility. Today, when female fertility can be explored accurately with a minimally invasive procedure, such as TVE [4], and a reliable treatment exists for many major disorders, a prolonged waiting period is outdated [16].
It is concluded that in women with previously normal cycles infertility should be investigated already after a 6-month period of fertility-focused intercourse and that transvaginal endoscopy, which combines minihysteroscopy and transvaginal hydrolaparoscopy, can be proposed as a first-line technique.
Care Womens Centre is one of the Best Fertility hospital in Indore. We are a highly successful IVF center in Indore. In our Fertility Hospital, we offer all types of investigation and treatment under one roof. Our hospital has the most affordable IVF center in Indore with all advanced equipment and highly skilled doctors. Besides the treatment, a balanced lifestyle and stress management also plays an important part. At our Best fertility hospital, we also stress on lifestyle and stress management before any further advanced treatments. Book an appointment call now 8889016663 or visit https://www.carewomenscentre.com for more information.
Eat more complex(“Slow”) carbs and limit highly processed ones. Your body digests bad carbs (like cookies, cakes, white bread and white rice) quickly, and turns them into blood sugar.
For a fertility diet to improve egg quality, load your plate with fruit and veggies. To know more about #IVF call 88890–16663 or visit www.carewomenscentre.com for more details.
Transvaginal endoscopy (TVE) has recently been introduced as a useful method for the diagnosis of infertility in women [1]. By insertion of a 3.5 mm-diameter telescope through the posterior vaginal fornix, the fallopian tubes and the adnexae can easily be visualised and further investigated [2]. This method has been proposed for infertile women with low risk of pelvic abnormality, a rather normal gynecological history and normal sonographic appearance of the pelvis.
The traditional investigation of an infertile woman without suspicious history of pelvic adhesions or endometriosis is by hysterosalpingography (HSG). In patients with normal HSG results, induction of ovulation and artificial insemination with the husband’s sperm is usually proposed for 4–6 cycles. If no pregnancy is achieved, then laparoscopy and hysteroscopy follow. The development of small-diameter telescopes has promoted pain-free hysteroscopy as an office procedure and recommended its application in every infertile woman prior to any infertility treatment [3].
The application of TVE as a substitute for standard diagnostic laparoscopy has encouraged gynaecologists to consider changes in their recommendations for infertile women with no obvious pelvic abnormalities [4]. By the application of office hysteroscopy and TVE, the mechanical factor within the uterine cavity, the ostia, and the proximal and distal part of the tubes can be eliminated, and no infertility treatments are given without complete diagnosis [5].
TVE can verify pelvic micro- and filmy adhesions and foci of endometriosis, which are not visible with standard laparoscopy [6]. Also, the small-diameter telescope can be inserted within the fibria (fibrioscopy) and propagated to the endosalpinx (infundibulum), enabling evaluation of the distal part of the salpinx. The diagnostic advantages of TVE over traditional laparoscopy, and which patients have an indication for TVE, are still under evaluation, and more studies are needed to draw final conclusions [4].
The aim of our study was to evaluate and compare the performance, diagnostic potential and the results of TVE at the initial learning period of five gynaecology groups in three different countries.
Patients and methods
Patients
We performed TVE between 1 January 1999 and 13 July 2001 on 78 infertile patients. Their average age was 33 (32–34) years, and the mean number of years of their infertility problem was 3.7 (3–5) years. We recruited three groups of patients. Group A comprised 46 patients that were operated on in Milan and Bologna, in Italy. Group B contained ten patients in Ioannina, Greece, and group C was composed of 22 patients in Nicosia, Cyprus. All patients were selected to be at minimal risk of pelvic adhesions, and vaginal sonography verified uterus and ovaries to be normal. The first four patients of each group were examined by laparoscopy, to evaluate the potential of the technique and minimise risks for the patients.
Method
The procedure of TVE was followed as published by Gordts et al. [7]. In the operating room the patients were placed in the lithotomy position, and a drip infusion was administrated. Heavy sedation was used as anaesthesia. After the patient had undergone disinfection with aqueous chlorhexidine solution, hysteroscopy was performed. A metallic cannula was then adjusted to the cervical os for the use of chromotubation. The cervix was lifted with a tenaculum placed on the posterior lip, and, in some cases, the central part of the posterior vaginal fornix was infiltrated with 2 ml of 1% lidocaine. The Veress needle was introduced 1.5 cm below the cervix and inserted into the pelvic cavity. Approximately 200 ml of warm saline solution was introduced into the pouch of Douglas. A 3 mm blunt trocar was inserted by a stab incision in the posterior fornix; then, a 2.7 mm-diameter rigid endoscope was used, with an optical angle of 30°, attached to a video-camera. The saline irrigation continued throughout the procedure to keep the bowel and tubo-ovarian structures afloat. The posterior of the uterus and the tubo-ovarian structures were carefully observed, and tubal passage, using indigo-carmine, was confirmed. In some cases the infundibulum of the endosalpinx could be visualised.
Results
All 78 patients tolerated TVE very well, and no cancellations were reported. The average time of the whole procedure was 30 min. Hospitalisation days varied, being 4 h for group C, 48 h for group A and 24 h for group B. No long-term postoperative complications or infections were reported. Trocar entry complications, pain and bleeding were reported in one patient in group C and two in group B, which stopped after pressure. Postoperative bleeding was reported in one patient in group B, which stopped after the port entry in the vaginal vault had been sutured. One patient in group B had a bowel perforation, which was diagnosed early and treated conservatively with antibiotics.
The visualisation of the tubo-ovarian structures was reported in all cases in group A, in 7/10 (70%) cases in group B and in 17/22 (77%) cases in group C. The TVE findings are shown in Table 1 and differed in each department. In 30–50% of the cases normal pelvic findings were reported. The rate of pelvic endometriosis diagnosed ranged from 9% to 20%, and the overall frequency of adhesions was 20%.
The number of CO2 laparoscopies needed to verify the diagnosis made by TVE ranged from 7% to 10%, as shown in Table 2. The overall number of patients who avoided having to have CO2 laparoscopy, by undergoing TVE, was 41/78 (51%). The remainder of the patients, 30/78 (38.5%) after the diagnosis was established by TVE, needed to undergo either further surgery for adhesiolysis or IVF treatment.
Discussion
This study presents the initial application and the results of the new method of TVE in three countries. All units demonstrated similar high diagnostic potential and minimal complication rates in the TVE procedure and wide acceptability of the method by the patients. The fact that patients underwent this procedure under heavy sedation, and that the average time of inspection was half an hour, minimised hospital stay and increased acceptability by the patients for the proposed TVE procedure. The time of hospitalisation after TVE varied enormously among the three groups and was decided in advance by every department separately, depending on their protocol rather than on the real need of patients’ hospitalisation. Since TVE is a new method, the safety of the method should be secured.
The observation of micro- and filmy adhesions and foci of endometriosis seen by TVE and otherwise missed by CO2 laparoscopy makes its application attractive [8]. In patients aged close to 40 years and under pressure to achieve a pregnancy as soon as possible, it seems reasonable to reassure the woman about the fertility potential prior to her undergoing any trials with ovulation induction by ruling out the 20% chance that she might have a mechanical problem. The simplicity, safety and accuracy of the results of TVE encourage the routine application of this method in infertile women [9].
Bowel injury is one of the risks encountered when the Veress needle and then the trocar are inserted into the vaginal vault [10]. Usually, the diagnosis of wrong entry is immediate, and conservative management with antibiotics is, in most cases, enough. Usually, these injuries are very rare and are avoided by the careful selection of patients and by experience.
Transvaginal endoscopy also has its limitations, as it is not possible for the gynaecologist to inspect the anterior part of the uterus, or the anterior pelvic peritoneum [4]. Nor is it possible for the abdominal cavity to be investigated in the way CO2laparoscopy does. However, by gaining experience, the gynaecologist can clearly recognise the appendix, omentum and even adhesions below the umbilicus. It is essential to understand that selection of patients for TVE is absolutely necessary in the first cases. Also, women suspected of having pelvic adhesions and /or needing operative laparoscopy should be excluded from TVE. The learning of the TVE technique is relatively easy, especially for gynaecologists who perform traditional laparoscopy and hysteroscopy.
When TVE and hysteroscopy methods are applied as a first choice of evaluation for all infertile woman, some hesitation arises as to whether this can be performed as an office procedure, as proposed by Gordts et al. [5] and Brosens et al. [9]. The high rate of adhesions, 20% reported in these early studies and also found by us, probably indicates the performance of TVE/hysteroscopy in the operating room, whereas operative laparoscopy can follow for patients requiring further treatment. Of course, such an option can be always discussed and settled with the patient prior to the procedure. Recent technological advances provide trocars with a working channel, and minimal surgery can be performed by TVE [11]. Further evaluation of the potential of these new instruments is necessary to exact any conclusion.
The experience of the initial steps in learning TVE in the above-mentioned units in three Mediterranean countries demonstrates that this new method of investigating female infertility is feasible, gives accurate results and is easy to learn. It is of low cost and very well accepted by the patients. The risks for perioperative complications are minimal, depending on the surgeon’s experience and selection of the patients.
Are you looking for the Best fertility hospital in indore? Care Womens Centre is India’s world class Infertility Treatment hospital and IVF center in Indore Madhya Pradesh, easily accessible via all forms of transportation. A location convenient for IVF patients as they usually need to visit the hospital more frequently than other categories of patients. Led by internationally acclaimed IVF specialist Dr Shweta Kaul Jha, the team of Fertility Experts with professional qualifications and experienced expertise offer guarantee of success at a fraction of the price you would pay for similar treatments abroad.
The Best Infertility hospital, Care Womens Centre offers the complete range of infertility related treatments such as IVF, IUI, ICSI, test tube baby treatment and infertility treatment in Indore Madhya Pradesh. Our primary goal is to remedy a situation that prevents couples from becoming proud parents. Book an appointment https://www.carewomenscentre.com and call us 8889016663.