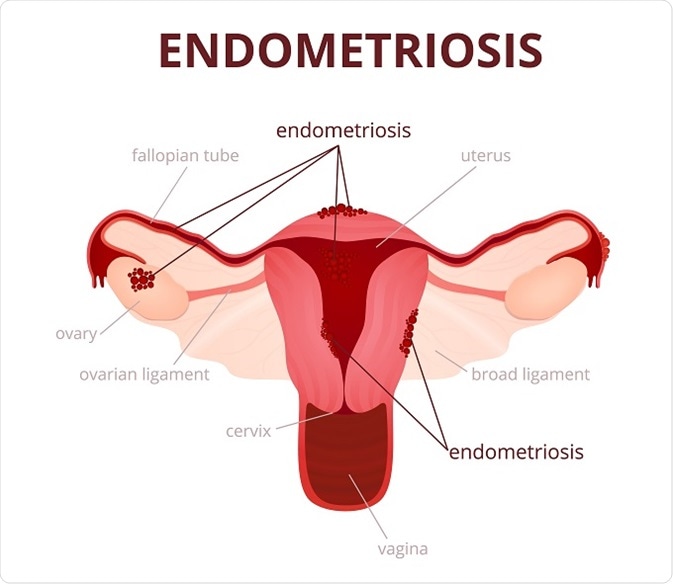
Endometriosis is a common disorder of the female reproductive organs and is the leading cause of chronic pelvic pain in women.
In women who have endometriosis, tissue similar to the lining of the uterus (endometrium) develops in other areas of the body, most commonly within the pelvic area or the abdominal cavity. The endometrial tissue may attach itself to the ovaries, the outside of the uterus, the intestines, or other abdominal organs. Rarely, endometriosis occurs outside the abdominal cavity, such as in the brain or lungs. Endometriosis may also develop in surgical scars following surgery on pelvic organs. The term “implant” is used to refer to a specific area of endometriosis in a certain tissue.
Endometriosis may not produce specific symptoms and signs, and most women with the condition don’t have any. However, women who have endometriosis and experience symptoms and signs they may include:
Pelvic pain that worsens just before a woman’s period (menstruation).
Pelvic pain that increases during menstration and gets better when her period ends.
Pain during sexual intercourse
Infertility
Many American women will experience problems with endometriosis, but an exact determination of the number of women affected is difficult, since many women may have the condition and do not have symptoms. In other situations, women may also have symptoms that could be attributed to endometriosis, but never undergo formal diagnostic studies to confirm that the condition is present. Most women who are diagnosed with endometriosis are between 25 and 35 years of age. Women may have symptoms for years before a definitive diagnosis is made.
During pelvic surgery for any gynecologic condition, about 1% of women are observed to have endometriosis. The percentages are much higher in young women undergoing laparoscopic surgery for pelvic pain and in women undergoing laparoscopic surgery to evaluate infertility.
Endometriosis is more common in Caucasian women than in African American or Asian women. Studies have also reported that endometriosis tends to occur most commonly in taller, thin women with a low body mass index (BMI).
Women with first-degree relatives who have endometriosis are also more likely to develop the condition, suggesting that the genes a woman inherits from her parents can sometimes predispose her to develop endometriosis.
Are you looking for the best Fertility centre and Test tube baby center in Indore? if yes so Care Womens Centre is a leading one of the best Test tube baby center and Best fertility hospitals in Indore. Dr Shweta Kaul Jha is one of the best IVF specialists in Indore at Care Womens Centre, that provide the 80% successful infertility treatment in Indore. She is also one of the eminent and renowned doctors in the field of gynecology and infertility treatments. She is one of the first infertility specialists of the city who had full-fledged structured training to understand and treat reproductive medicine which includes reproductive endocrinology, endoscopic treatment and IVF/ICSI treatments. Book an appointment call now 8889016663 and visit https://www.carewomenscentre.com/ for more information.
A fertility specialist is usually an obstetrician-gynecologist (specialist in women’s reproductive health) with advanced education, research, and professional skills in reproductive endocrinology. These highly trained and qualified doctors are the specialists to see about infertility.
Couples may want to talk to a health care professional for a referral to a clinic where doctors and staff have this special training. In addition, fertility clinics often have specialized equipment and imaging technology needed to make a diagnosis and to do semen testing and other specialized tests right at the office.
Check the American Society for Reproductive Medicine for a specialist and clinic in your area. A primary care physician or gynecologist will also be able to refer you to a fertility clinic.
Infertility is a problem that involves both partners. Therefore, the infertility specialist evaluates both the woman and the man. Testing for infertility is usually not done until after the couple has tried to become pregnant for at least 1 year if the woman is younger than 35 years, or older than 35 years and have not conceived during a six-month period of trying.
How Is Infertility Diagnosed?
Medical history A health care professional will take a complete medical history. Couples may be asked to provide the following information:
Complete medical history for both the man and the woman
Whether the woman has never been pregnant (primary infertility) or has been pregnant and is now unable to conceive (secondary infertility)
How long has the couple been trying to become pregnant
History of the woman’s previous pregnancies, if any
How often the couple has intercourse
A woman’s menstrual history
Current medical treatment for the man and woman
Physical examination
A health care professional may perform a physical examination on both partners, including the following aspects:
Routine blood pressure, pulse, and temperature
Height and weight
Inspection of sexual organs
Hormone testing
Woman: Pelvic ultrasound scan to look for masses, cervical mucus testing
Man: Genital examination, testicle size, hernias
A health care professional will discuss the findings from the medical history and physical examination. Sometimes, a complete infertility evaluation may take up to two menstrual cycles before the factors causing the infertility can be found.
Further testing for men
The male partner will be asked to submit a semen sample for a complete semen analysis. Even though a man has fathered a child in the past, he will still be asked to submit a semen sample because his reproductive system may have changed.
The semen sample may be collected at the laboratory (in a private room through masturbation). If a sample is collected at home, it must be collected in a sterile plastic container and delivered to the lab at a body temperature no more than 60 minutes after ejaculation.
Some men cannot produce a semen sample through masturbation. Therefore, the sample can be collected through intercourse, using a special non-spermicidal condom provided by the laboratory. For best results, the semen sample should be collected 3 to 5 days after a period of having no sexual intercourse.
A man may produce no sperm for various reasons. He may produce few sperm or sperm that have defects that prevent them from reaching or fertilizing the egg.
Further testing for women
Several conditions may affect a woman’s ability to get pregnant. A health care professional will evaluate the entire reproductive system.
The cervix plays a key role in the transport of the sperm after intercourse. Cervical mucus production, amount, and characteristics change according to the estrogen concentration depending on the menstrual cycle.
The uterus is the final destination for the embryo and the place where the fetus develops until delivery. Therefore, the uterus may be associated with primary infertility or with pregnancy problems and premature delivery. Other problems affect the development and function of the uterus (specifically the endometrium or inner layer of the uterus).
Ovaries may not release eggs. Fallopian tubes may be blocked. The doctor will want to evaluate all parts of the reproductive system.
The health care professional may use any of several procedures to examine the woman’s reproductive organs:
Pelvic exam: This is a general physical examination in which the doctor feels the uterus for detectable masses and views the cervix.
Hysterosalpingogram: This is an imaging study of the uterus and Fallopian tubes after contrast dye has been injected through the cervix. It shows the shape of the uterus and if the Fallopian tubes are open. The dye appears white on an X-ray. This test is usually performed before ovulation so the dye does not disrupt an egg or developing embryo. The woman may be given pain medication before the test because some women experience minor pain.
Ultrasound: Pelvic ultrasound has become an important tool in the evaluation and monitoring of infertile women. It is a way to detect uterine fibroids, endometrial polyps, ovarian cysts, and other abnormalities in the pelvis from the outside with sound waves. A sonohystogram, or saline infusion sonography (SIS) is a test that combines ultrasound with saline solution injected into the uterus.
Magnetic resonance imaging (MRI): This is another imaging procedure similar to an X-ray that uses magnetic waves to create images of the internal organs.
Hysteroscopy: This is a method of directly seeing the interior of the uterus with an instrument.
Laparoscopy: This is a surgical procedure that allows the doctor to see directly inside the pelvis with tiny instruments inserted through small cuts in the abdomen.
Endometrial biopsy: This test involves removal of a small piece of tissue from the uterine lining by a catheter inserted through the cervix. This test can help determine whether the menstrual cycle is normal and whether ovulation has occurred.
Infertility may be caused by so many different problems that it is beyond the scope of this discussion to outline them all.
Care Womens Centre is one of the best fertility centres in Indore. We are specialist in providing infertility treatment in Indore through the revolutionary method IVF. Our center is known for its world best treatment and the affordable cost of the treatment that makes the infertility treatment accessible for everyone. Dr Shweta Kaul Jha is a renowned reproductive IVF specialist in Indore at Care Womens Centre. We are providing the best treatments with the top- notched techniques and the latest methods used for IVF such as egg donation, sperm donation, IUI, test tube baby treatment Blastocyst techniques that maximize the success rates by many folds. Book an appointment call now 8889016663 and visit https://www.carewomenscentre.com/ for more information.
Infertility is the inability of a couple to become pregnant (regardless of cause) after 1 year of unprotected sexual intercourse (using no birth control methods).
Infertility affects men and women equally.
Most infertility cases are treated with medication or surgery.
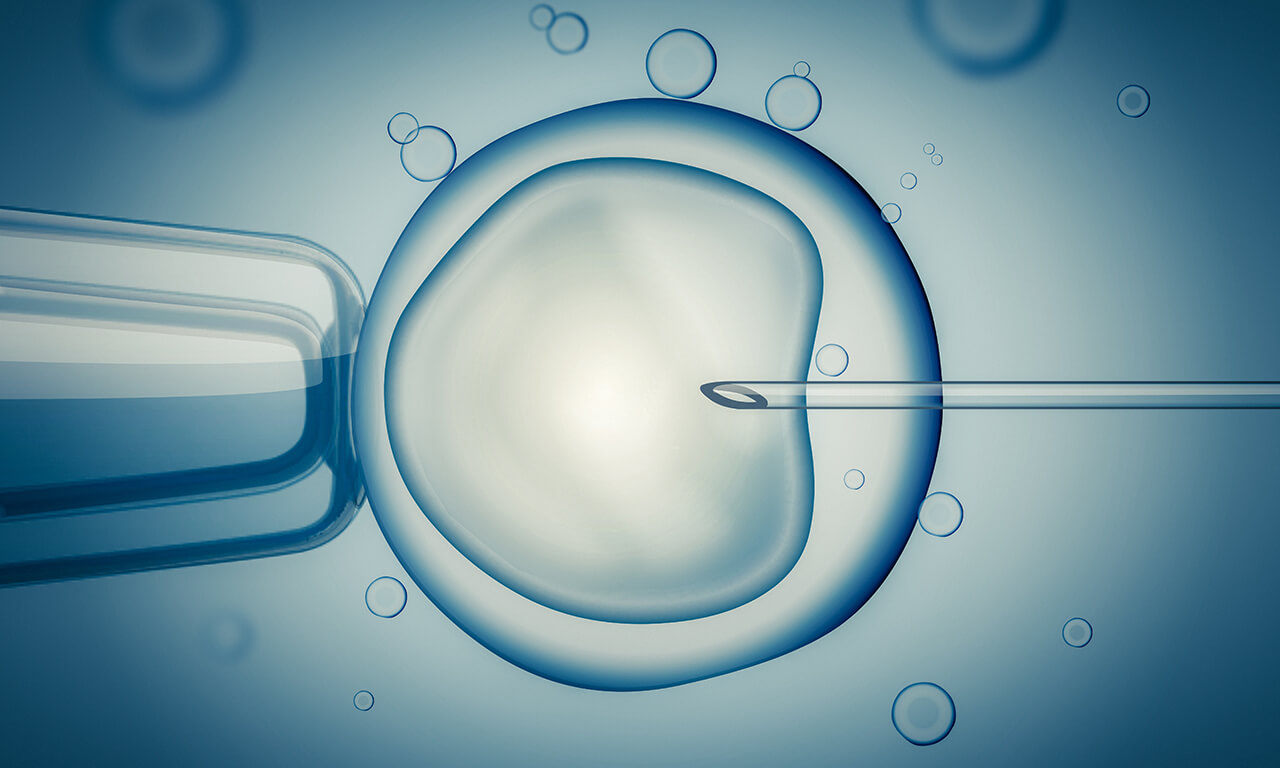
Improvements in fertility treatment have made it possible for many women whose male partner is infertile to become pregnant. These new and advanced technologies include in vitro fertilization (IVF), intracytoplasmic sperm injection (ICSI), and other similar procedures.
What Causes Infertility?
The normal reproduction process requires interaction between the female and male reproductive tracts. The woman ovulates and releases an egg from her ovaries to travel through the Fallopian tube to her uterus (womb). The male produces sperm. Both egg and sperm normally meet in the woman’s Fallopian tube, where fertilization occurs. The embryo then implants in the uterus for further development.
Infertility occurs when something in this pattern does not happen. The problem could be with the woman (female infertility), with the man (male infertility), or with both. Unknown factors cause infertility 10% of the time. For infertility with an unknown cause, all findings from standard tests may be normal. The actual cause of infertility may not be detected because the problem may be with the egg or sperm itself or with the embryo and its inability to implant.
Pelvic inflammatory disease (PID)
Sexually transmitted diseases, namely, gonorrhea and Chlamydia, may be associated with pelvic inflammatory disease (PID) and damage a woman’s Fallopian tubes. A health care professional can detect pelvic inflammatory disease using cultures or molecular biologic studies of vaginal discharge and blood testing for sexually transmitted diseases. If a woman does not recall ever having pelvic inflammatory disease, her doctor m
ay be able to see scarring or blockage of the tubes during a surgical procedure called laparoscopy. Tiny cameras and instruments are inserted through small cuts in the abdomen to allow the doctor to view the reproductive organs.
Endometriosis
Endometriosis affects women during their reproductive years and may contribute to infertility. It can cause pelvic pain and infertility. A woman may be at risk for developing it if she has a family history of the disease. With endometriosis, uterine lining tissue grows outside the uterus and may damage the ovaries and Fallopian tubes. A woman may not know she has a mild form of this condition. Sometimes the doctor finds it during laparoscopy.
Environmental and occupational factors
Certain environmental factors may cause men to produce a less concentrated sperm. Exposure to lead, other heavy metals, and pesticides have been associated with male infertility. Many other factors, such as excessive heat exposure, microwave radiation, ultrasound, and other health hazards, are more controversial as to whether they induce infertility.
Toxic effects related to tobacco, marijuana, and other drugs
Smoking may cause infertility in both men and women. In experimental animals, nicotine has been shown to block the production of sperm and decrease the size of a man’s testicles. In women, tobacco changes the cervical mucus, thus affecting the way sperm reach the egg
Marijuana may disrupt a woman’s ovulation (release of the egg). Marijuana use affects men by decreasing the sperm count and the quality of the sperm.
Heroin, cocaine, and crack cocaine use induces similar effects but places the user at increased risk for pelvic inflammatory disease and HIV infection associated with risky sexual behavior.
In women, the effects of alcohol are related more to severe consequences for the fetus. Nevertheless, chronic alcoholism is related to disorders in ovulation and, therefore, interferes with fertility. Alcohol use by men interferes with the synthesis of testosterone and has an impact on sperm concentration. Alcoholism may delay a man’s sexual response and may cause impotence (unable to have an erection).
Exercise
Exercise should be encouraged as part of normal activities. However, too much exercise is dangerous, especially for long-distance runners. For women, it may result in disruption of the ovulation cycle, cause no menstrual periods, or result in miscarriages (loss of pregnancy). In men, excessive exercise may cause a low sperm count.
Inadequate diet associated with extreme weight loss or gain
Obesity is becoming a major health issue in the United States. Obesity has an impact on infertility only when a woman’s weight reaches extremes.
Weight loss with anorexia or bulimia can create problems with menstrual periods (no periods) and thyroid levels, thus disrupting normal ovulation.
Age
A woman becomes less fertile as she ages into her fifth decade of life (age 40-49 years). Among men, as they age, levels of testosterone fall, and the volume and concentration of sperm change.
Healthy couples younger than 30 years who have regular sexual intercourse and use no birth control methods have a 25% to 30% chance of achieving pregnancy each month. A woman’s peak fertility is early in the third decade of life. As a woman ages beyond 35 years (and particularly after age 40 years), the likelihood of becoming pregnant is less than 10% per month.
The aim of this study was to explore the benefits of in vitro fertilization (IVF) for patients and hospitals under different protocols and if IVF treatment should be incorporated into health care.
PERSPECTIVE:
The government should consider including IVF treatment in health insurance. Hospitals and patients could obtain the best benefit by following the hospital’s recommended protocol.
SETTING:
This retrospective study was conducted from January 2014 to August 2017 at an academic hospital.
METHODS:
A total of 7440 patients used gonadotropin-releasing hormone agonists (GnRHa) protocol, 2619 patients used, gonadotropin-releasing hormone antagonists (GnRHant) protocol, and 1514 patients used GnRHa ultra-long protocol. Primary outcomes were live birth rate (LBR), cost-effectiveness, hospital revenue, and government investment.
RESULTS:
The cycle times for the GnRHa protocol and the GnRHa ultra-long protocol were significantly higher than the GnRHant protocol. Patients who were ≤29 years chose the GnRHant protocol. The cost of a successful cycle was 67,579.39 ± 9,917.55 ¥ and LBR was 29.25%. Patients who were >30 years had the GnRHa protocol as the dominant strategy, as it was more effective at lower costs and higher LBR. When patients were >30 to ≤34 years, the cost of a successful cycle was 66,556.7 ± 8,448.08 ¥ and the LBR was 31.05%. When patients were >35 years, the cost of a successful cycle was 83,297.92 ± 10,918.05 ¥ and the LBR was 25.07%. The government reimbursement for a cycle ranged between 11,372.12 ± 2,147.71 ¥ and 12,753.67 ± 1,905.02 ¥.
CONCLUSIONS:
The government should consider including IVF treatment in health insurance. Hospitals recommend the GnRHant protocol for patients <29 years old and the GnRHa protocol for patients >30 years old, to obtain the best benefits. Patients could obtain the best benefit by using the protocol recommended by the hospital.
Does the perception of failure without a solution or way forward of infertile couples have a mediator role between the importance couples attribute to parenthood and depressive symptoms?
SUMMARY ANSWER:
The perception of failure without a solution or way forward, assessed by feelings of entrapment and defeat, mediates the effect of the importance of parenthood on depressive symptoms of infertile men and women.
WHAT IS KNOWN ALREADY:
Research has documented that the heightened importance of parenthood affects infertile couples’ adjustment to infertility and medical treatments. However, it remains unclear which psychological mechanisms and perceptions may underlie the association between having parenthood as a nuclear aspect of life and presenting depressive symptoms related to difficulties in accomplishing that important life goal. Although these links have been scantly addressed in infertility, previous studies have pointed to the role that perceptions of defeat and entrapment have in several psychopathological conditions.
STUDY DESIGN, SIZE, DURATION:
The study was cross-sectional. Couples pursuing medical treatment for their fertility problems were invited to participate by their doctors in several public and private clinics. Data collection took place between July 2009 and 2011.
PARTICIPANTS/MATERIALS, SETTING, METHODS:
One hundred forty-seven infertile couples consented to participate in the study. Both couple members (147 women and 147 men) completed a set of self-report instruments for the assessment of depressive symptoms, perceptions of defeat and entrapment, importance of parenthood and rejection of a childfree lifestyle. Analyses were conducted through Structural Equation Modeling and followed a dyadic analysis strategy, allowing for controlling the interdependence of the data.
MAIN RESULTS AND THE ROLE OF CHANCE:
The hypothesized tested model showed a very good fit to the data [(χ(2) = 68.45, P = 0.014, comparative fit index = 0.98, standardized root-mean-square residual = 0.06 and root mean square error of approximation = 0.06] and explained 67 and 58% of the variability in depressive symptoms in women and men, respectively. Results revealed that the importance of parenthood does not have a direct effect on depressive symptoms of infertile men and women, but an indirect effect, by affecting the perception of having failed and not being able to solve it or move forward [women: estimate for indirect effect: 0.38 (bias corrected (BC) 95% confidence interval (CI) = 0.25; 0.56; P < 0.001); men: estimate for indirect effect: 0.23 (BC 95% CI = 0.06; 0.40; P = 0.013)].
LIMITATIONS, REASONS FOR CAUTION:
The study was cross-sectional, which does not allow for the establishment of causality. Another limitation is the heterogeneity of the sample, as participants were recruited at various stages of their fertility care. In addition, due to the specific nature of the variables, further studies are needed to establish exactly how the relationship between defeat and entrapment and depression operates, as the mechanism may be bidirectional.
WIDER IMPLICATIONS OF THE FINDINGS:
This study emphasizes the role of perceptions of defeat and entrapment on the psychological adjustment to infertility and assisted reproduction. These emotional processes should be taken into consideration and targeted in psychological interventions of couples undergoing medical treatments for infertility. In fact, although parenthood may be perceived as a core purpose for many couples dealing with difficulties in conceiving, it is only when these difficulties are experienced as failures without a resolution and as inescapable, that couples are prone to develop depressive symptoms.
The truth is, being a parent is a life changer; it offers couples an entirely different perspective on why they wake up every day. And people who are deprived of this blessing can come to Care Womens Centre. Care Womens Centre is one of the Best fertility hospitals in Indore to get IVF treatments and fulfill their inherent desire to be a parent. Care Womens Centre is provide the world class infertility treatment, test tube baby treatment, IUI treatment and ICSI treatment in Indore. Dr Shweta Kaul Jha is Best IVF specialist at Care Womens Centre. If you are Search for the Best centre for IVF in Indore come to Care Womens Centre. Book an appointment today call now +918889016663 and visit https://www.carewomenscentre.com for more information.
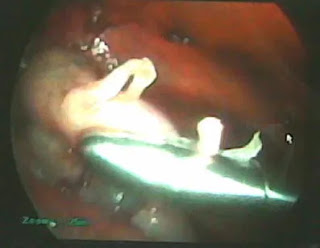
We report a case of a live twin birth after laparoscopic treatment of a ruptured heterotopic pregnancy. A 29-year-old woman, with a history of right salpingectomy for ectopic pregnancy, became pregnant after transfer of three embryos at in vitro fertilization treatment. At the ninth week of gestation, she was admitted to our clinic with abdominal pain. Ultrasonographic examination revealed a triplet heterotopic pregnancy consisting of an intrauterine twin pregnancy and an ectopic pregnancy in the left fallopian tube. An immediate laparoscopy was planned and left salpingectomy was performed. In the postoperative period, intrauterine twin pregnancy continued uneventfully; at the 35th week of gestation, two healthy infants with birth weights of 2,206 and 2,426 g were delivered. Heterotopic pregnancies must be kept in mind after assisted reproductive techniques. Early diagnosis allows successful laparoscopic treatment without sequel. Laparoscopic surgery is an appropriate method to manage selected patients with heterotopic tubal pregnancy.
Introduction
Ectopic pregnancy (EP) refers to the implantation of a viable ovum outside the uterine corpus. Heterotopic pregnancy (HP) is the simultaneous occurrence of gestations at two or more implantation sites. It is most often manifested as concomitant intrauterine pregnancy (IUP) and EP [1]. Although EP is not uncommon in women of reproductive age, HP is rare in the general population, with an incidence of 1:7,963–30,000 in spontaneous conceptions [2]. The increased incidence of pelvic inflammatory disease (PID), the common usage of ovulation inducing agents, and assisted reproductive techniques (ART) have contributed to the increasing incidence of both multiple gestations and HP in the last decade. The rate of HP after in vitro fertilization (IVF) has been reported to be as high as 1% [2, 3], although it’s true incidence is unknown. Most recent studies exhibit the incidence about 152 per 100,000 pregnancies in ART cycles [4]. Due to the difficulty in the diagnosis, rupture of the tube, bleeding, and the need for emergency operations are seen more often in heterotopic than in ectopic pregnancies. Thus, all pregnancies as a result of ART must be evaluated cautiously. Here, we report a triplet heterotopic pregnancy, which was successfully diagnosed and treated by laparoscopy.
Case A 29-year-old woman G: 1, P: 0, with unexplained infertility, not to be able to conceive for 3 years, underwent an IVF procedure. She had a history of an EP 3 years ago treated by unilateral right salpingectomy. After initial downregulation using leuprolide acetate 500 μg/day (Lucrin; Abbott, Cedex, Istanbul, Turkey), 225 IU/day of recombinant follicle stimulating hormone (Gonal F; Serono Laboratories) was given starting from the second day of the menstrual cycle. When at least three follicles >17 mm were observed, human chorionic gonadotropin (hCG; Pregnyl; Organon, Cambridge, UK) was administered 10,000 IU i.m. and oocyte retrieval was performed at 35.5 h. Five of eight retrieved oocytes were successfully fertilized by IVF. Two days after oocyte retrieval, three embryos were transferred. Luteal phase support in the form of intravaginal micronized progesterone was given. Serum beta-hCG was 52 IU/mL on day 12 and we deduced intrauterine live twin pregnancy 4 weeks after embryo transfer.
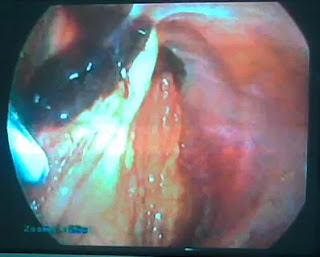
At the ninth week of gestation, she was admitted with abdominal pain. Transabdominal ultrasonography (US) examination revealed intrauterine live twin pregnancy and a left-sided ectopic pregnancy with fetal heart beat. The vital signs of the patient were in normal range. A diagnostic laparoscopy was performed using general anesthesia and the ports were placed in classical locations carefully to protect the uterus. A ruptured left tubal EP was found covered with omentum hanging on the anterior abdominal wall (Figs. 1 and 2). Left salpingectomy was performed successfully. The patient was discharged at the second day after the operation. In the postoperative period, the intrauterine twin pregnancy continued uneventfully with no unusual aspect of the prenatal care and she delivered two healthy infants at the 35th week of gestation with birth weights of 2,206 and 2,426 g.
Discussion
HP is a rare entity in spontaneous cycles; however, its incidence has risen with the widespread use of ART. Although most ectopic gestations in HPs occurring after ART are tubal, 10.8% are extratubal [5] and more difficult to diagnose. The beta-hCG may continue to rise normally and US may be unreliable in the presence of a normal intrauterine gestation especially in HPs. The intermittent unilateral pain can be attributed to a hemorrhagic corpus luteum, or a small degree of ovarian hyper stimulation [6]. Therefore, we need to have better evaluation of the adnexa when pain is out of proportion of what is expected in a woman with IUP. Most cases are missed on their initial examination, and patients frequently present with symptoms of rupture before the diagnosis is ultimately made, as in this case. Therefore, keeping its high incidence after ART in mind, careful surveillance of extrauterine structures at the first US examination is essential in pregnancies achieved after ART.
Different mechanisms may predispose to development of HP after ART cycles. More embryos transferred by ART procedures increase both multiple gestation and EP incidences [7]. Other factors predisposing to ectopic gestation are previous tubal damage caused by PID, endometriosis and tubal surgery, previous ectopic pregnancy, and ovulation induction. The hormonal milieu at the moment of transfer has been proposed as possible causes as well [8]. Thus, it seems more important to limit the number of embryos transferred, particularly in patients who present risk factors for HP and in young women, thereby minimizing the risk of EP.
Concerning the prognosis of the IUP, favorable outcomes are reported in 50–60% of cases [2]. In HPs, spontaneous or induced abortions are more likely to occur than with intrauterine-only pregnancies; however, birth outcomes are similar, when an intrauterine gestation of a heterotopic pregnancy results in a live birth [9].
Management of HP should be conservative if possible; the primary goal is removal of the EP, while preserving the intrauterine pregnancy. Several treatment modalities have been described, either surgical or medical. The choice of treatment depends mainly on the hemodynamic condition of the patient, localization of the ectopic pregnancy, and desire for the ongoing pregnancy and future pregnancies.
The safety of laparoscopy during pregnancy has been well documented [1]. The advantages of laparoscopy compared with laparotomy in postoperative recovery are well known [1]. Laparoscopy allows prompt diagnosis and treatment, thereby providing good outcome avoiding the postoperative inconvenience of laparotomy, and has the advantage of an immediate result compared with medical treatment. In our case, the pregnancy was not affected by the operation and resulted with delivery of healthy twins.
Moreover, every physician dealing with ART should be aware of the possibility of HP, even in the absence of any predisposing risk factors. A high index of suspicion followed by an early surgical laparoscopic intervention can minimize maternal morbidity and preserve continuing IUP.
Welcome to one of India’s premium fertility hospitals, Care Womens Centre. The joy of holding a new born is every couple’s dream. But not all are lucky, as many issues can keep them from experiencing this joy. Care Womens Centre is one of the Best Fertility hospitals and IVF centers in indore. we providers the best infertility treatment in Indore. We, at Care Womens Centre, offer couples a chance to address their issues and increase chances of starting a family! We follow ethical practices and provide patients the best care to make sure they walk out with a smile on their face. Book an appointment call now 8889016663 or visit https://www.carewomenscentre.com/ for more information.
आइवीएफ तकनीक — यह एक तकनीक ही नहीं बल्कि एक वरदान के रूप में आगे आ राह है , आज कल देर से विवाह एक आम बात है । करियर की भागदौड मैं सब उलझे चले जा रहे है।शादी के बाद भी लंबे समय तक शिशु को जन्म न देने का निर्णय और तनावग्रस्त जीवनशैली आगे चलकर दंपतियों में निःसंतानता का बडा कारण बनता जा रहा है।
यदि आप निःसंतान दम्पति है तो तुरंत केयर वूमेन सेंटर मैं आकर हमारे फर्टिलिटी एक्सपर्ट से संपर्क करे। अधिक जानकारी के लिए कॉल करें 88890–16663 या व्यक्तिगत परामर्श हेतु विजिट करे 203, विशाल अस्त्र , सत्य साई स्क्वायर , विजय नगर , इंदौर |
Miscarriage doesn’t mean that you can never have a baby.
For more information, kindly call: 88890–16663 or visit www.carewomenscentre.com for more details.
Best fertility hospital in indore, ivf specialist in indore, test tube baby center in indore, ivf treatment cost in indore, Best centre for IVF in indore, affordable ivf cost in indore, infertility treatment in indore, ivf center in indore, fertility centre in indore, ICSI treatment in indore